Halting the Allergic March: Is it Possible?
Allergic diseases have been on the rise for the past few decades, being tagged as one of the epidemics of the 20th century.1 This has greatly impacted the overall health and socioeconomic status of those who suffer from it.
Atopy, derived from the Greek word “ατοπια” meaning “out of place” or “strange disease” was introduced in 1923 by American allergists Coca and Cooke to describe a familial tendency to becoming sensitized to certain substances like house dust mites, or food and develop hypersensitivity reactions.2,3 Atopy was used to describe the atopic family of diseases, specifically allergic asthma, allergic rhinitis (AR) and atopic dermatitis (AD).
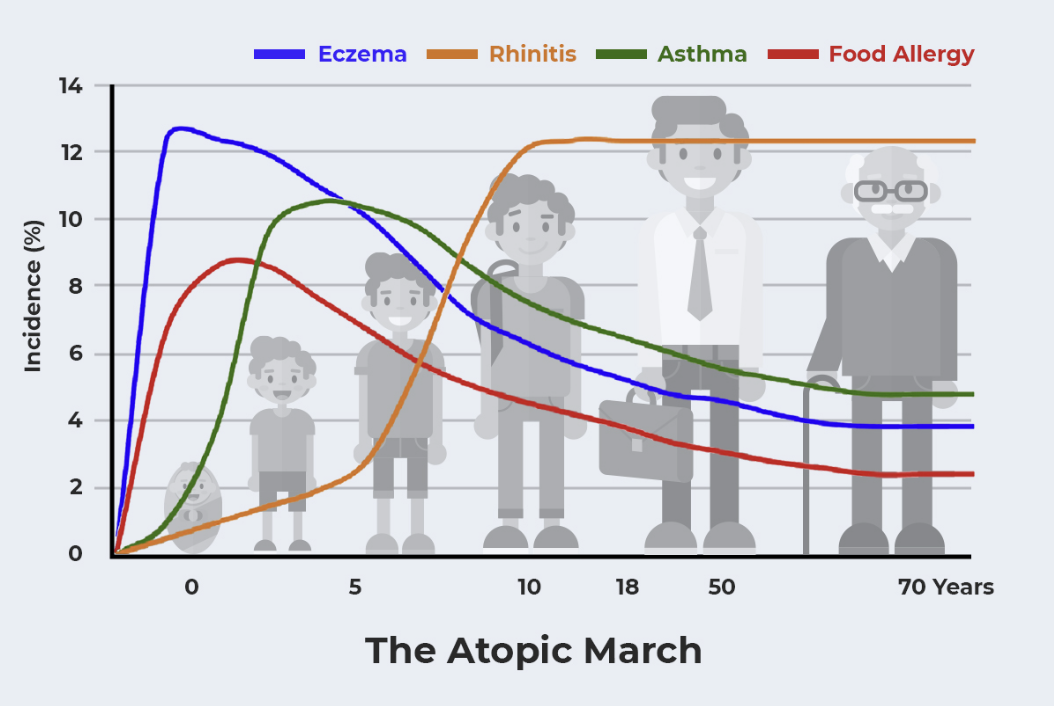
Now, the atopic march or allergic march refers to the natural history or course of allergic diseases as they develop during infancy or early childhood.4 It explains the apparent progression of allergic diseases from AD to allergic asthma and then to AR (Figure 1).5 One interesting facet is that the presence of one allergic condition may increase the risk for the development of others, resulting in the additive feature of the atopic march.6
Figure 1. The atopic march. AD prevalence peaks early in infancy, opening the door for the consequent development of the atopic march. Development of food allergy, asthma, and AR in the young toddler age group is common after cutaneous manifestations.5
Being aware of the allergic march helps us take care of our patients in a number of ways. First, it alerts the family and physician that asthma is likely to occur. This could make it easier for us to recognize asthma early and prevent delays in management. Second, awareness heightens the family’s and physician’s suspicion in looking for possible precipitants of disease (e.g. food allergies or wheezing with colds). Third, and perhaps most importantly, as efforts move toward disease prevention, the atopic march holds the promise of a reliable early marker to identify those most at risk and most likely to benefit from prevention.7
Despite its seemingly simple definition, quite a number of articles have been written about the allergic march and one of the questions raised is that, do all patients follow the classical march sequence or can they “skip around”?8
In a review article by Gabryszewski and Hill, they discussed more than one trajectory of the allergic march. Data from the Children’s Hospital of Philadelphia showed that although the path of “AD to allergic asthma to AR” may be the most common, this was only seen in a small percentage of children and that multiple pathways, with the latest addition of eosinophilic esophagitis (EoE) exist.9
Nevertheless, available data tells us that in a subset of children, impairment of the skin barrier results in the development of AD. This facilitates cutaneous sensitization which increases the risk of systemic allergic responses.10 The link between AD and allergic airway diseases is influenced by the age of AD onset and its severity.
The goal of preventing the progression of the atopic march is one of the “holy grails of allergy”11, preventing atopic disease, and the increase in the prevalence of the atopic disease has resulted in a greater need for prevention.
In a Keystone Symposium in 2020, the main objective was to present and discuss potential microbial-epithelial-immune interactions underlying the early life origins of allergic disorders, as well as immune mechanisms that might suggest novel disease prevention or intervention strategies12 – ways to possibly halt the allergic march or the progression from AD to asthma and rhinitis.
Figure 2. Damage to epithelial surfaces underlies the various manifestations of allergic disease and the possible interventions to prevent them.12
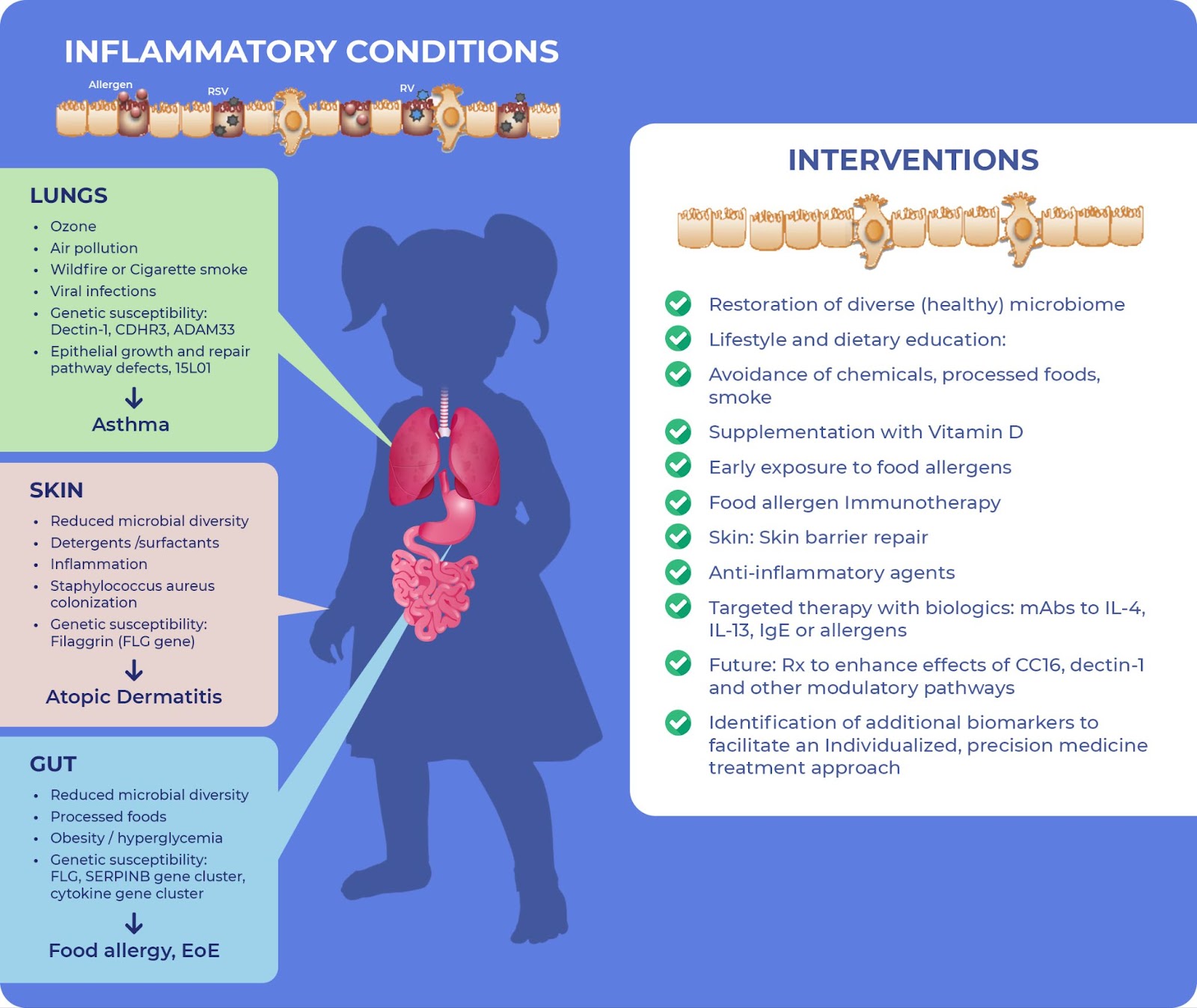
Figure 2 summarizes how the epithelia of the skin, lungs and gut act as critical sensors of environmental stimuli and are assaulted by various stimuli including an altered microbiome, air pollution, food allergens in a changed diet, chemicals in modern detergents, and plastics. These exposures lead to changes of lungs, skin, or gut epithelial surfaces, driving a type 2 immune response that regulates atopic diseases.12
The right-hand side of the figure highlights interventions to prevent the development and progression of allergic disease, including early exposure to food allergens (as seen in the LEAP & EAT studies) to promote oral tolerance and a diverse microbiome. Other measures include oral immunotherapy with food allergens leading to desensitization.12
The concept of skin barrier dysfunction occurring in AD suggests the importance of early skin care even before clinical eczema appears.13 Several pilot studies have looked into daily emollient therapy in high-risk infants, showing a reduction in incidence of AD. However, larger studies such as the BEEP study (Barrier Enhancement for Eczema Prevention) on 1,394 newborns at high risk for AD who applied emollient daily for 1 year, showed no difference in occurrence or severity of AD.11
Targeted therapy with biologics including monoclonal antibodies such as dupilumab in children as young as 6 months old, to limit the effects of IL-4, IL-13, IgE, and even allergens themselves are also being studied.11
There is now more evidence to support the idea that the allergic march is not just one path, but an “umbrella term” for multiple pathways due to the heterogenous description of atopic diseases.14
AD is oftentimes the first manifestation of the allergic march and a better understanding of the mechanisms leading to it is needed to help improve preventive measures of the atopic march and help bring our allergy patients a better life in the 21st century.
References:
- Kemp AS, et al. The allergy epidemic: what is the Australian response? Medical Journal of Australia. 2006 Aug 21;185(4):226–227.
- Wüthrich B (ed). The atopy syndrome in the third millenium. Curr Probl Dermatol. 1999;28:1-8.
- Aw M, et al. Atopic March: Collegium Internationale Allergologicum Update 2020. Int Arch Allergy Immunol. 2020;181:1–10.
- Spergel JM and Paller AS. Atopic dermatitis and the atopic march. J Allergy Clin Immunol. 2003;112(6 Suppl):S118-S127.
- Czarnowicki T, et al. Novel concepts of prevention and treatment of atopic dermatitis through barrier and immune manipulations with implications for the atopic march. J Allergy Clin Immunol. 2017;139:1723-34.
- Hill DA and Spergel JM. The atopic march: Critical evidence and clinical relevance. Ann Allergy Asthma Immunol. 2018 Feb;120(2):131-137.
- Busse WW. The atopic march: Fact or folklore? Ann Allergy Asthma Immunol. 2018 Feb;120(2):116-118.
- Tran MM and Sears MR. Can the atopic march be predicted? Ann Allergy Asthma Immunol. 2018;120(2):115–116.
- Gabryszewski SJ and Hill DA. One march, many paths: Insights into allergic march trajectories. Ann Allergy Asthma Immunol. 2021;127:293–300.
- Johansson E and Hershey GKK. Contribution of an impaired epithelial barrier to the atopic march. Ann Allergy Asthma Immunol. 2018 Feb;120(2):118-119.
- Jimenez J and Paller AS. The atopic march and its prevention. Ann Allergy Asthma Immunol. 2021;127:289–290.
- DeKruyff RH, et al. Summary of the Keystone Symposium "Origins of allergic disease: Microbial, epithelial and immune interactions," March 24-27, Tahoe City, California. J Allergy Clin Immunol. 2020 Apr;145(4):1072-1081.e1.
- Leung DYM, et al. Cutaneous barrier dysfunction in allergic diseases. J Allergy Clin Immunol. 2020 Jun;145(6):1485-1497.
- Maiello N, et al. New directions in understanding atopic march starting from atopic dermatitis. Children. 2022;9:450.